Case is presented by Dr. Uma Rani G, Associate Professor, Department of Anatomy, JIMS Homoeopathic Medical College.
ABSTRACT:
Homoeopathy is a study which is based on individualisation and constitutional makeup. Present case study on anal fissure is the example which reflects the principle of homeopathy. The present case study reviews the most common anorectal disorder, anal fissure. Anal fissure is one of the very frequent and painful proctologic diseases. Even though anal fissure is not a major life threatening disease, the unbearable pain in anus, because of which patient presents himself to the doctor for consultation, advice and treatment. Homoeopathy offers the safe, rigour, effective and permanent treatment, for such cases.
KEYWORDS:
Anal fissure, Homoeopathy, Constitutional remedy, Individualisation, Physical generals, Mental symptoms.
INTRODUCTION:
Anal fissure is one of the most painful conditions among the anorectal disorders. Trauma to the anoderm with the passage of a hard stool is thought to be a common initiating factor. The pain sensation is out of proportion to the trauma. The pathophysiology of anal fissures is not entirely clear. It is probable that an acute injury leads to local pain and spasm of the internal anal sphincter.. There is immense scope for anal fissures to heal itself naturally with aid of homoeopathic medicines, with slight modification in life style and few dietary measures. Most commonly, anal fissures occur in the posterior midline; however, in up to 25% of women and 8% of men, a fissure can be located in the anterior midline. In patients who have lateral fissures, the clinician should consider an alternative aetiology such as Crohn’s disease, malignancy, tuberculosis, or HIV infection.
AETIOLOGY: The smooth lining of the anal canal is soft and elastic in nature so as to allow stool to pass. It is hairless and full of small nerve endings. Therefore it is quite sensitive to touch and pain. That is precisely why fissures are quite painful. Anal fissures are caused by injury or trauma to the anal mucosa. This trauma may result from hard or large stools.
• It may also occur due to repeated diarrhoea or constipation when one has to strain a lot to pass stool.
• It may also occur during labour when there may be a tear in the perineal region.
• Occasionally insertion of rectal thermometer or a colonoscope or during enema.
• In other cases HIV, anal cancer, syphilis, leukemia or TB may cause an anal fissure.
• There is also the possibility of anal fissure being caused by the presence of inflammatory bowel diseases like Ulcerative Colitis or Crohn’s disease.
PATHOLOGY: An anal fissure is either acute or chronic. The upper internal end of the fissure stops at the dentate line .Because the fissure occurs in the stratified sensitive epithelium of the lower half of the anal canal, pain is the most prominent symptom.
CLINICAL FEATURES:
•Pain, sometimes severe, during and after bowel movements that can last up to several hours. Due to the pain, there is anal sphincter spasm, which makes constipation still worse.
•Bright red blood on the stool or toilet paper after a bowel movement.
• Itching or irritation around the anus.
• Malodorous discharge may occur due to the discharge of pus from the fissure.
• In chronic fissure a skin tag, or small lump of skin, next to the tear is seen called as sentinal pile.
DIAGNOSIS AND EXAMINATION FINDINGS: The diagnosis can typically be confirmed by physical examination and anoscopy in the orifice if tolerated by the patient. By gentle separation of the buttocks and examination of the anus, a linear separation of the anoderm can be identified at the lower half of the anal canal. On digital examination, chronic fissure feels rough, raised, or fibrotic in the mid-distal anal canal and a skin tag, called sentinal pile also visible.
PREVENTION:
An anal fissure can’t always be prevented, but you can reduce your risk of getting one by taking the following preventive measures:
• Keeping the anal area dry.
• Cleansing the anal area gently with mild soap and warm water.
• Avoiding constipation by drinking plenty of fluids, eating fibrous foods, and exercising regularly.
• Treating diarrhoea immediately.
• Changing diapers frequently (for infants).
HOMOEOPATHIC APPROACH:
Homeopathy offers the most definitive treatment for this excruciatingly painful condition. Homeopathic treatment for Anal Fissure eliminates the tendency of recurrence of the fissure. It provides the most wholesome, complete relief from this obstinate condition. Our approach is always through process of Individualisation.
FEW IMPORTANT HOMOEOPATHIC REMEDIES FOR ANAL FISSURES:
Nitric Acid: Top Homeopathic medicine for treatment of Anal Fissures
Calcarea phoshoricum : for chronic non healing fissure.
Graphites: for fissures occurred due to severe constipation with soreness of anus.
Ratanhia : for fissures with severe burning pain in anus which is temporary relieved by cold water.
Silicea: for fissure due to hard stool that has to be removed mechanically.
Sulphur : is the best Homeopathic medicine when the stool is hard and dry, causing tears and immense pain in the anus while passage.
Bryonia, Alumina and Natrum Mur: relieving Anal Fissure constipation
CASE:
Mrs. Shailaja, 28yrs, Female, Resident of Dilsukhnagar at Hyderabad came with complaints of Pain in Rectum during and after passing stool since 3years. <sitting, > by moving about. Constipation since 3years.
History of presenting complaint: Complaints started 3years back after haemorrhoids operation, Complaints started insidiously. Pain severe, burning cutting type, during pain pt cannot sit, frequent urging for stool, straining at motion agg the pain, pt try to remove the stool mechanically, to relieve pain pt puts ice pieces into the anus, even though there was no relief. Occasionally trace streaks of blood in stool.
Past history of illness: Pt had endometriosis, Adenomyosis and hysterectomy done before 3months back. Pt had lt sided ovarian cyst, and left ovary has removed while hysterectomy. Pt also has pulmonary stenosis, pt also had history of rheumatic fever at the age of 16years. Haemorrhoids begins during 2nd pregnancy and underwent surgery 3years back.
Treatment history: Pt taken allopathic and Homoeopathic and Ayurvedic treatment without much improvement.
Family history: Oral, GI cancer history in close relatives. Father died with heart complaint
Personal history: Studied up to 10th standard. she has 2 children, elder one suffering from allergic asthma. Financially stable. No addictions and habits.
Menstrual history : Before hysterectomy menses usually late, scanty, LBA.
Obstetrical history : G2P2L2A0D0 , No Complications during both pregnancies.
Mental Generals: Pt is very impatient, irritable during complaints, Patient is usually very friendly but when complaints occur pt become irritable, impatient, despair of recovery. Wants to be alone. Very sensitive to comments made by other. Jealous, egoist. Pt won’t get anger easily, if pt got anger very difficult to control, pt will throw the things, tears the cloths. Violent burst of anger.
Physical Generals: Appetite moderate. Thirsty pt. B/M obstinate constipation, frequent urging but difficult to pass it, severe pain develop on straining in toilet, Stool large, very dry and hard, passing stool relieves the pt temporarily. Sleep- disturbed. Hot pt, hot sensation all over the body. Desire fanning always. Prefers mild warm food and drinks. Desire tea. Desire juicy things. General left sided complaints.
General Examination: Pt is mild over weight, fair, robust constitution. Pulse: 80/m. Heart rate: 80/m, BP : 130/90mmhg.
Local examination: Very dry around anal area, cracks visible, sentinal pile visible.
Investigation: Not done particularly.
Provisional diagnosis: By clinical symptoms, and history of past illness Provisionally diagnosed as ‘Fissure in ani’
Miasmatic Diagnosis: Syco syphilitic.
Totality of symptoms:
• Pain in Rectum during and after stool <sitting and >by moving about.
• Stool removes mechanically.
• Constipation obstinate.
• Frequent urging for stool, stool very hard and dry,
• Pt is very impatient.
• Irritable during complaints,
• Patient is usually very friendly but when complaints occur pt become irritable, impatient, depair of recovery.
• Wants to be alone ,Very sensitive to comments made by other. Jealous, egoistic.Pt won’t get anger easily, if pt got anger difficulty to control, pt will throw the things, tears the cloths. Violent burst of anger.
• Appetite moderate.
• Thirsty pt.
• B/M obstinate constipation, frequent urging but difficult to pass it, severe pain develop on straining in toilet,
• Stool large, very dry and hard, passing stool relieves the pt tempororly.
• Sleep- disturbed
• Hot pt , hot sensation all over the body.
• Desire fanning always.
• Prefers mild warm food and drinks.
• Desire tea.
• Desire juicy things.
• General left sided complaints.
RUBRICS SELECTED:
1. MIND – SENSITIVE – external impressions, to all
2. MIND – JEALOUSY
3. MIND – EGOTISM
4. MIND-ANGER
5. GENERALS – FOOD and DRINKS – juicy things – desire
6. GENERALS – SIDE – left – then right side
7. GENERALS – FOOD and DRINKS – tea – desire
8. RECTUM – CONSTIPATION – removed mechanically; stools have to be
9. RECTUM – PAIN – STOOL- during
10. RECTUM – PAIN – STOOL- after
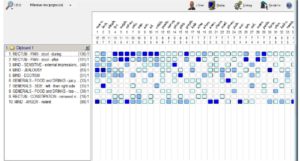
PROBABLE REMEDIES:
- Nux – 15/8 ,
- Lach – 15/7,
- Staphy-11/7 ,
- Lyco -11/6 ,
- Sulph-10/6 ,
- acid-11/4.
PRESCRIPTION:
Rx; 1.Nux.vom 200 1dose
. 2..S.L for 2days.
FOLLOW UP:
After three days Pt came and reported no change in condition, severe pain , constipation ,pt can not sit also, she is becoming mad, violent, anger during pain.
Rx; 1. Staphysagria 200 1dose.
- S.L for 1week. Pt asked to wait for at least 1week,
Next day pt called me and told about large faecal matter passed out, pain also greatly relieved. Now pt is very comfortable. After one week Pt came and reported regularly passing stool no pain and constipation.
Rx; 1. S.L for 2weeks.
Staphysagria :
- It covers miasm ie syco-syphilitic.
- Multiple pathology in middle aged female, mainly related to uterus.
- Mental symptoms suited exactly.
- Right time pt receives right prescription, that’s why no return of complaints till now.
References:
1. Das. S A concise text book of surgery 8th edition, published by Dr.S.Das, Kolkata, India
2. Harrison’s principles of internal medicine, 18th edition, vol 2, Mc Graw Hill Publishers, India.
3. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4076876/
4. Boericke’s New Manual of Homeopathic Materia Medica with REPERTORY Third Revised & Augmented Edition Based on Ninth Edition
5. Boenninghausen’s Characteristics Materia Medica & Repertory with word index by Dr. C.M. Boger
6. Kent JT. Repertory of Homeopathic Materia Medica. Reprint Edition. New Delhi: B. Jain Publishers (P) Ltd.; 2007.
7. NashE.B. Leaders in Homoeopathic Therapeutics. Therapeutic index. Available from: http://www.homeoint.org/books2/nashtherap/theraindex.htm