Case Presentation:
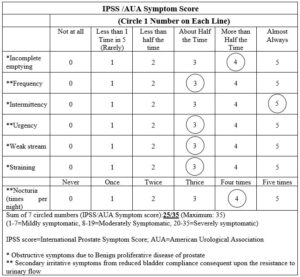
Mr. RKS (Reg. no: R-00644-12083/P-329), a seventy-four-year-old diabetic male patient consulted on 1.8.2007 for the treatment of increased nocturnal urinary frequency (D/N: 3-4/4-5) with urgency, hesitancy, poor and obstructed flow of urine with straining and not get done feeling since many years. He was taking Glyzid M for diabetes and was prescribed Urimax D, Duprost, Normoprost, Hytrin and Riconia in the past by Allopathic physicians which gave only partial relief in symptoms. His initial IPSS score (International Prostate Symptom Score) was 25/35. He was advised ultrasonography of prostate which he got done the same day.
Initial IPSS (1.8.07):
|
IPSS /AUA Symptom Score |
||||||
|
(Circle 1 Number on Each Line) |
||||||
|
Not at all |
Less than 1 Time in 5 (Rarely) |
Less than half the time |
About Half the Time |
More than Half the Time |
Almost Always |
|
|
*Incomplete emptying |
0 |
1 |
2 |
3 |
5 |
|
|
**Frequency |
0 |
1 |
2 |
4 |
5 |
|
|
*Intermittency |
0 |
1 |
2 |
3 |
4 |
|
|
**Urgency |
0 |
1 |
2 |
4 |
5 |
|
|
*Weak stream |
0 |
1 |
2 |
4 |
5 |
|
|
*Straining |
0 |
1 |
2 |
4 |
5 |
|
|
Never |
Once |
Twice |
Thrice |
Four times |
Five times |
|
|
**Nocturia (times per night) |
0 |
1 |
2 |
3 |
5 |
|
|
Sum of 7 circled numbers (IPSS/AUA Symptom score):25/35 (Maximum: 35) (1-7=Mildly symptomatic, 8-19=Moderately Symptomatic, 20-35=Severely symptomatic) IPSS score=International Prostate Symptom Score; AUA=American Urological Association * Obstructive symptoms due to Benign proliferative disease of prostate ** Secondary irritative symptoms from reduced bladder compliance consequent upon the resistance to urinary flow |
||||||
Investigation:
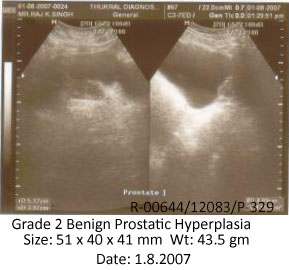
Initial USG prostate (1.8.07):
Prostate is moderately enlarged measuring 51 x 40 x 41 mm with weight of approx. 43.5 gms s/o grade 2 benign prostatic hypertrophy. Dense calcification is seen within prostatic parenchyma leading to non-visualization of inferior outline of prostate. Post void residual urine is approx. 31.8 cc.
INITIAL USG REPORT and FILM
By personality assessment of the patient, following rubrics were selected for repertorisation with the help of Complete repertory using Hompath software.
Rubrics for repertorisation:
- Ailment from business cares
- Dreams of business of the day
- Dreams of unsuccessful efforts
- Anxiety about health
- Quiet disposition
- Confusion of mind
- Generalized weakness
- Tendency to catch cold
- Urination frequent
- Urination profuse
Repertorisation chart:
Result of repertorisation:
|
Remedies |
Acid phos |
Calc c |
Puls |
Nux v |
Sepia |
|
Totality |
21 |
20 |
18 |
17 |
17 |
|
Symptoms covered |
10/10 |
10/10 |
9/10 |
9/10 |
9/10 |
Selection of remedy:
After repertorial analysis, the similimum was selected on the basis of ailments from business cares, dreams of business of the day and dreams of unsuccessful efforts which indicated Acid phosphoricum.
Date-wise follow up:
1.8.07: Acid phosphoricum 30 twice a day. Sabal serrulate Q, 10 drops TDS x 4 weeks.
9.9.07: Nocturnal urinary frequency, urgency, hesitancy reduced. Flow improved. Same prescription x 4 weeks.
29.10.07: Better than before. His IPSS score was 17/35. Same prescription x 6 weeks.
Follow up IPSS (29.10.07):
|
IPSS /AUA Symptom Score |
||||||
|
(Circle 1 Number on Each Line) |
||||||
|
Not at all |
Less than 1 Time in 5 (Rarely) |
Less than half the time |
About Half the Time |
More than Half the Time |
Almost Always |
|
|
*Incomplete emptying |
0 |
1 |
2 |
4 |
5 |
|
|
**Frequency |
0 |
1 |
3 |
4 |
5 |
|
|
*Intermittency |
0 |
1 |
2 |
4 |
5 |
|
|
**Urgency |
0 |
1 |
3 |
4 |
5 |
|
|
*Weak stream |
0 |
1 |
3 |
4 |
5 |
|
|
*Straining |
0 |
1 |
3 |
4 |
5 |
|
|
Never |
Once |
Twice |
Thrice |
Four times |
Five times |
|
|
**Nocturia (times per night) |
0 |
1 |
2 |
4 |
5 |
|
|
Sum of 7 circled numbers (IPSS/AUA Symptom score):17/35 (Maximum: 35) (1-7=Mildly symptomatic, 8-19=Moderately Symptomatic, 20-35=Severely symptomatic) IPSS score=International Prostate Symptom Score; AUA=American Urological Association * Obstructive symptoms due to Benign proliferative disease of prostate ** Secondary irritative symptoms from reduced bladder compliance consequent upon the resistance to urinary flow |
||||||
18.12.07: Urgency, hesitancy much reduced. Urinary frequency became almost normal (D/N: 3-4/2). Flow much improved. Same prescription x 8 weeks.
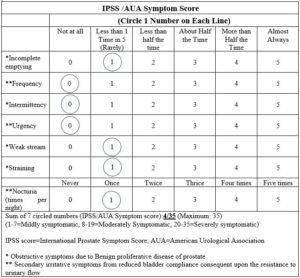
20.5.2008: Patient was supposed to report by the end of February but he returned for follow up in May and told that he was totally asymptomatic. His IPSS score was 4/35.
Final IPSS (25.5.08):
|
IPSS /AUA Symptom Score |
||||||
|
(Circle 1 Number on Each Line) |
||||||
|
Not at all |
Less than 1 Time in 5 (Rarely) |
Less than half the time |
About Half the Time |
More than Half the Time |
Almost Always |
|
|
*Incomplete emptying |
0 |
2 |
3 |
4 |
5 |
|
|
**Frequency |
1 |
2 |
3 |
4 |
5 |
|
|
*Intermittency |
1 |
2 |
3 |
4 |
5 |
|
|
**Urgency |
1 |
2 |
3 |
4 |
5 |
|
|
*Weak stream |
0 |
2 |
3 |
4 |
5 |
|
|
*Straining |
0 |
2 |
3 |
4 |
5 |
|
|
Never |
Once |
Twice |
Thrice |
Four times |
Five times |
|
|
**Nocturia (times per night) |
0 |
2 |
3 |
4 |
5 |
|
|
Sum of 7 circled numbers (IPSS/AUA Symptom score):4/35 (Maximum: 35) (1-7=Mildly symptomatic, 8-19=Moderately Symptomatic, 20-35=Severely symptomatic) IPSS score=International Prostate Symptom Score; AUA=American Urological Association * Obstructive symptoms due to Benign proliferative disease of prostate ** Secondary irritative symptoms from reduced bladder compliance consequent upon the resistance to urinary flow |
||||||
On repeat ultrasonography of prostate dated 20.5.08, the size of prostate was 43 x 27 x 32 mm and weight 19.7 gms which is normal.
Final USG prostate (20.5.08):
FINAL USG REPORT and FILM
Inference:
The patient was clinically asymptomatic and IPSS score reduced from 25/35 to 4/35. He was advised to stop the treatment and report in case of any trouble.


Testimonial Dr.Girish Gupta
I was introduced to her by Dr Kulbhushan Bharadwaj of New Delhi two months ago. It is surprising how could Dr. Kavitha organize my webinar on “Evidence-based Homoeopathy in Dermatology” in such a short span of time. It shows her dedication and commitment to promote homoeopathy even during the Corona pandemic.
She is also publishing an online newsletter to give academic homoeopathic physicians a chance to share their evidence-based cases. This is again a praiseworthy initiative. Pooling and sharing of knowledge is the need of the hour.
I can only say that Dr Kavitha Kukunoor is a “Garland maker” because she is making a huge garland of budding as well as full bloom homoeopaths to spread the fragrance of homoeopathy around the globe. Long live Dr. Kavitha and KHA.
Dr Girish Gupta, MD (Hom), PhD Chief Consultant, Gaurang Clinic and Centre for Homoeopathic Research, Lucknow, India